MDMA is Different Than Psilocybin — But How?
Stephanie Karzon Abrams, Clinical neuropharmacologist | Clinical Director Mystic Health | Founder, Beyond Consulting | Research Director, Microdosing Collective 501c3
Updated for 2026
Originally published February 14, 2024 | Revised April 2026
It feels appropriate to have first written about the so-called "love drug" on Valentine's Day. Two years later, with meaningful shifts in the regulatory landscape and an ever-growing body of clinical research, it's time to revisit this piece — with clearer science and a more accurate picture of where things stand today.
Information about both MDMA's and psilocybin's ability to support symptoms of depression and boost serotonin continues to circulate widely. Although some effects can appear similar, these two compounds behave very differently in the brain. Here is an updated overview of how they differ mechanistically — and why that matters clinically.
First, Serotonin
Serotonin (5-HT) is often referred to as a "feel-good" neurotransmitter. It plays a role in regulating mood, anxiety, and happiness, among other physiological functions.
Serotonin receptors are found throughout the body, with significant concentrations in the central nervous system (CNS) — including the brain and spinal cord — where they play key roles in mood regulation, cognition, and pain perception. These receptors are also prevalent in the peripheral nervous system and various peripheral tissues.
In the gastrointestinal tract, serotonin is crucial for regulating motility and secretion. Approximately 90% of the body's serotonin (the molecule itself) is produced and stored here — which is why the gut is sometimes called the body's "second brain." Serotonin receptors are also found in blood vessels, platelets, the heart, and lungs, where they influence blood pressure, clotting, heart function, and respiratory regulation. The receptors are classified into several subtypes — 5-HT1 through 5-HT7 — each with specific distributions and functions, highlighting serotonin's broad physiological and psychological reach.
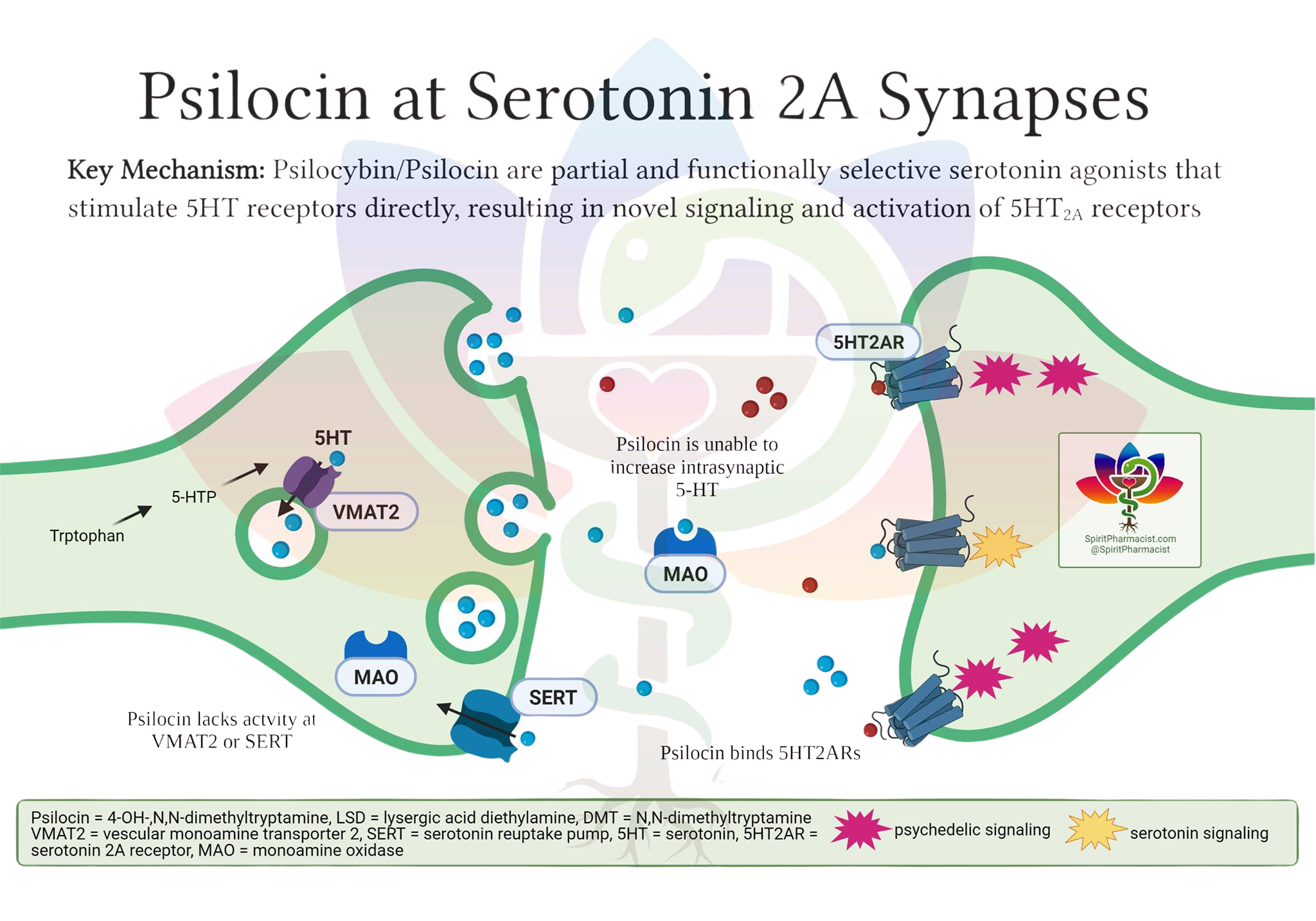
Psilocybin: A Direct Receptor Agonist
Psilocybin is a (partial) agonist of serotonin receptors (5HT-R), with highest affinity and functional activity at the 5-HT2A receptor.
This means that psilocybin — and more precisely its active metabolite, psilocin — binds to serotonin receptors and induces a positive biological effect. It does not cause the body to release more serotonin. Its primary action is receptor agonism, leading to downstream effects on neural circuits and neuroplasticity.
Psilocin closely resembles serotonin in molecular structure and fits into the same receptor "locks" in the brain. Think of it as a lock-and-key mechanism: serotonin (5-HT) is the natural key that binds to its own receptor (the lock). When psilocin binds to the 5-HT2A receptor, it directly activates it — triggering a cascade of changes in brain cell activity that produces the characteristic alterations in perception, mood, and thought associated with the psychedelic experience. This is not due to an increase in serotonin levels; psilocin is simply acting as a structural stand-in for serotonin at these specific receptors.
MDMA: An Indirect Serotonergic Agent
MDMA is not a direct agonist of serotonin receptors, but it does significantly increase serotonin availability.
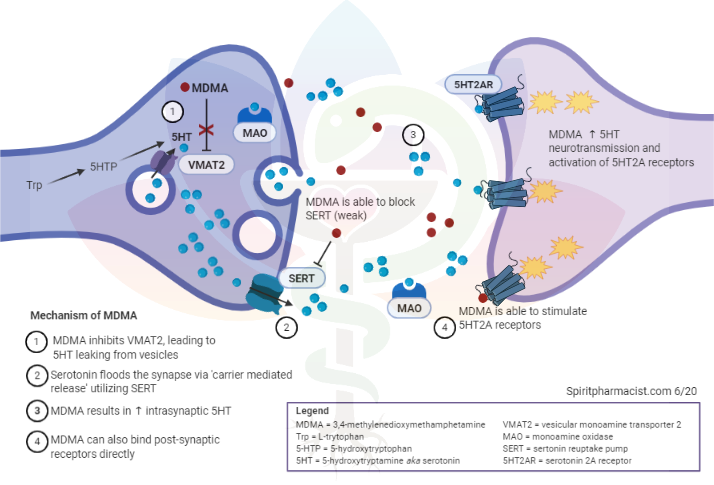
Rather than binding directly to the receptor, MDMA acts on the transporters responsible for recapturing serotonin and returning it to neurons for storage. These transporters are called SERT (serotonin reuptake transporters). By inhibiting SERT — and, importantly, reversing its direction of transport — MDMA causes a large flood of serotonin into the synaptic cleft, where it can then bind to and saturate receptors. This is the primary mechanism behind MDMA's characteristic emotional and prosocial effects.
MDMA also interacts with monoamine oxidase (MAO) pathways, which play a role in breaking down serotonin. While MDMA is not a classical MAO inhibitor in the pharmacological sense, this interaction is worth understanding in the context of drug safety — particularly regarding serotonin syndrome risk when MDMA is combined with prescription MAOIs (see below).
Serotonin syndrome is a potentially life-threatening condition resulting from excessive serotonin activity in the nervous system, often due to drug interactions or overdose. Symptoms can range from mild (shivering, diarrhea) to severe (muscle rigidity, fever, seizures). This risk applies to both MDMA and psilocybin when combined with MAOI-class medications, as serotonin metabolism is disrupted in both cases — though through different mechanisms.
MDMA's Broader Neurochemical Footprint
MDMA doesn't only affect serotonin — it also increases dopamine and norepinephrine.
This non-selectivity is actually one of the reasons MDMA has shown such promise in PTSD therapy. Psilocybin acts primarily through serotonergic pathways; MDMA's reach is broader.
Dopaminergic activity enhances mood and emotional engagement — both vital for therapeutic processes. Dopamine release during MDMA-assisted sessions can improve openness and emotional connection, facilitating exploration of traumatic memories and the development of positive associations.
Norepinephrine release increases arousal and emotional responsiveness, which can deepen affective processing during PTSD therapy sessions. It is also the reason you may feel your heart rate increase and body temperature rise — effects that are carefully monitored in clinical settings.
SSRIs and MDMA
When SSRIs are taken concurrently with MDMA, the SSRI's blockade of SERT can significantly inhibit MDMA's ability to flood the synaptic cleft with serotonin. Since SSRIs occupy these transporters to prevent serotonin reuptake, they also prevent MDMA from accessing and reversing those transporters. This leads to a marked reduction in MDMA's subjective effects.
SSRIs can also inhibit CYP2D6, an enzyme involved in MDMA metabolism, leading to increased plasma concentrations of MDMA. Despite higher blood levels, the expected psychoactive effects are diminished due to SERT blockade. This attenuation may prompt individuals to take more MDMA — potentially raising the risk of toxicity.
In summary: SSRIs blunt MDMA's effects by blocking SERT and reducing serotonin release, while simultaneously increasing MDMA plasma levels via CYP2D6 inhibition. The net result is reduced therapeutic and subjective response with increased cardiovascular and toxicological risk if dosage is escalated.
SSRIs and Psilocybin
Because psilocybin's mechanism is direct 5-HT2A receptor agonism rather than serotonin release, the interaction with SSRIs is different — and notably, not the mirror image of the MDMA case.
SSRIs increase synaptic serotonin over time, which leads to 5-HT2A receptor downregulation — the brain reduces receptor density in response to sustained stimulation. With fewer 5-HT2A receptors available, psilocin has less to bind to, resulting in a blunted psychedelic experience. This is distinct from simple competitive occupancy at the receptor; it is a longer-term adaptive change in receptor expression.
Clinically, those using psilocybin therapeutically while taking SSRIs may need a higher dose to achieve comparable effects. However — and this is an important nuance — preliminary data suggest that psilocybin's antidepressant efficacy may be preserved even when co-administered with SSRIs, with similar improvements in depressive symptoms and well-being observed in both medicated and unmedicated groups. These findings come from small, open-label, and survey-based studies; larger controlled trials are needed to confirm this.
Pharmacokinetic data show that SSRIs such as escitalopram do not significantly alter psilocin plasma levels, suggesting the interaction is primarily pharmacodynamic — occurring at the receptor level rather than in how the drug is metabolized.
In summary: SSRIs blunt the acute psychedelic experience of psilocybin, but may not significantly diminish its antidepressant efficacy. The combination appears generally tolerable, though rare adverse reactions are possible. Controlled studies are ongoing.
Recreation and Couples Therapy
MDMA has a long history in both recreational settings and underground therapeutic contexts. Known as an empathogen, it fosters feelings of emotional openness, love, and connection — from the dance floor to the therapy room. It has been used in informal couples work to support trust, acceptance, and the willingness to be vulnerable with a partner.
As clinical applications have evolved, interest in MDMA-assisted relationship therapy has grown — though it remains outside of formal approved indications.
MDMA, the FDA, and Where Things Stand in 2026
The regulatory path for MDMA-assisted therapy has been one of the most closely watched — and ultimately sobering — stories in psychedelic medicine over the past two years.
In 2024, Lykos Therapeutics (formerly MAPS PBC) submitted a New Drug Application (NDA) to the FDA for MDMA-assisted therapy for PTSD. The FDA convened an advisory committee in June 2024, which voted against recommending approval — raising concerns about trial design, functional unblinding, and the difficulty of separating drug effects from the psychotherapy component. The FDA issued a Complete Response Letter (CRL) in August 2024, declining to approve the application and requesting an additional Phase 3 trial.
Since then, Lykos has been navigating a path forward — including leadership changes and ongoing dialogue with the FDA about what a resubmission might require. As of early 2026, MDMA-assisted therapy for PTSD remains unapproved in the United States, though the research and advocacy infrastructure built by MAPS over decades continues to shape the field.
This does not diminish the strength of the underlying science or the lived experience of the many patients and therapists who have participated in trials. It does remind us that the road from breakthrough therapy designation to approval is rarely linear — and that rigorous methodology matters enormously.
I remain hopeful. For those using MDMA in underground therapeutic or recreational settings in the meantime: safety first, always.
Interested in how these compounds are being used clinically? Explore our COMP360 Psilocybin Readiness consulting or learn more about ketamine and psychedelic-assisted therapy clinic consulting.
References
Farré M, et al. Pharmacological Interaction Between MDMA and Paroxetine. J Pharmacol Exp Ther. 2007;323(3):954–62.
Tancer M, Johanson CE. Effects of Fluoxetine on MDMA in Humans. Psychopharmacology. 2007;189(4):565–73.
Liechti ME, et al. Acute Effects of MDMA Attenuated by Citalopram. Neuropsychopharmacology. 2000;22(5):513–21.
Liechti ME, Vollenweider FX. Neuroreceptors Mediating MDMA Effects. Hum Psychopharmacol. 2001;16(8):589–598.
Rietjens SJ, et al. Pharmacokinetics and Pharmacodynamics of MDMA. Crit Rev Toxicol. 2012;42(10):854–76.
Silins E, et al. Serotonin Syndrome, Ecstasy, and Serotonergic Substances. Aust N Z J Psychiatry. 2007;41(8):649–55.
Price CM, et al. SSRI Use and MDMA-Assisted Therapy for PTSD. J Clin Psychopharmacol. 2022;42(5):464–469.
Sarparast A, et al. Drug-Drug Interactions Between Psychiatric Medications and MDMA or Psilocybin. Psychopharmacology. 2022;239(6):1945–1976.
Gukasyan N, et al. Attenuation of Psilocybin Effects During SSRI/SNRI Use. J Psychopharmacol. 2023;37(7):707–716.
Barbut Siva J, et al. Classic Psychedelics and Serotonergic Antidepressants. J Psychopharmacol. 2024;38(2):145–155.
Sakai K, et al. Reddit Posts About SSRI and Psilocybin Coadministration. Psychopharmacology. 2024;241(8):1617–1630.
Erritzoe D, et al. Discontinuation of Antidepressants Prior to Psilocybin Therapy. J Psychopharmacol. 2024;38(5):458–470.
Goodwin GM, et al. Psilocybin for Treatment-Resistant Depression With Concomitant SSRI. Neuropsychopharmacology. 2023;48(10):1492–1499.
Becker AM, et al. Acute Effects of Psilocybin After Escitalopram Pretreatment. Clin Pharmacol Ther. 2022;111(4):886–895.
Malcolm B, Thomas K. Serotonin Toxicity of Serotonergic Psychedelics. Psychopharmacology. 2022;239(6):1881–1891.